 Dentist Referral Form
Dentist Referral Form 
André Hattingh
Vandeweghe S, Hattingh A, Wennerberg A, Bruyn HD.
J Oral Maxillofac Res. 2011 Oct 1;2(3):e1. doi: 10.5037/jomr.2011.2301.
PMID: 24421993
Abstract
OBJECTIVES:
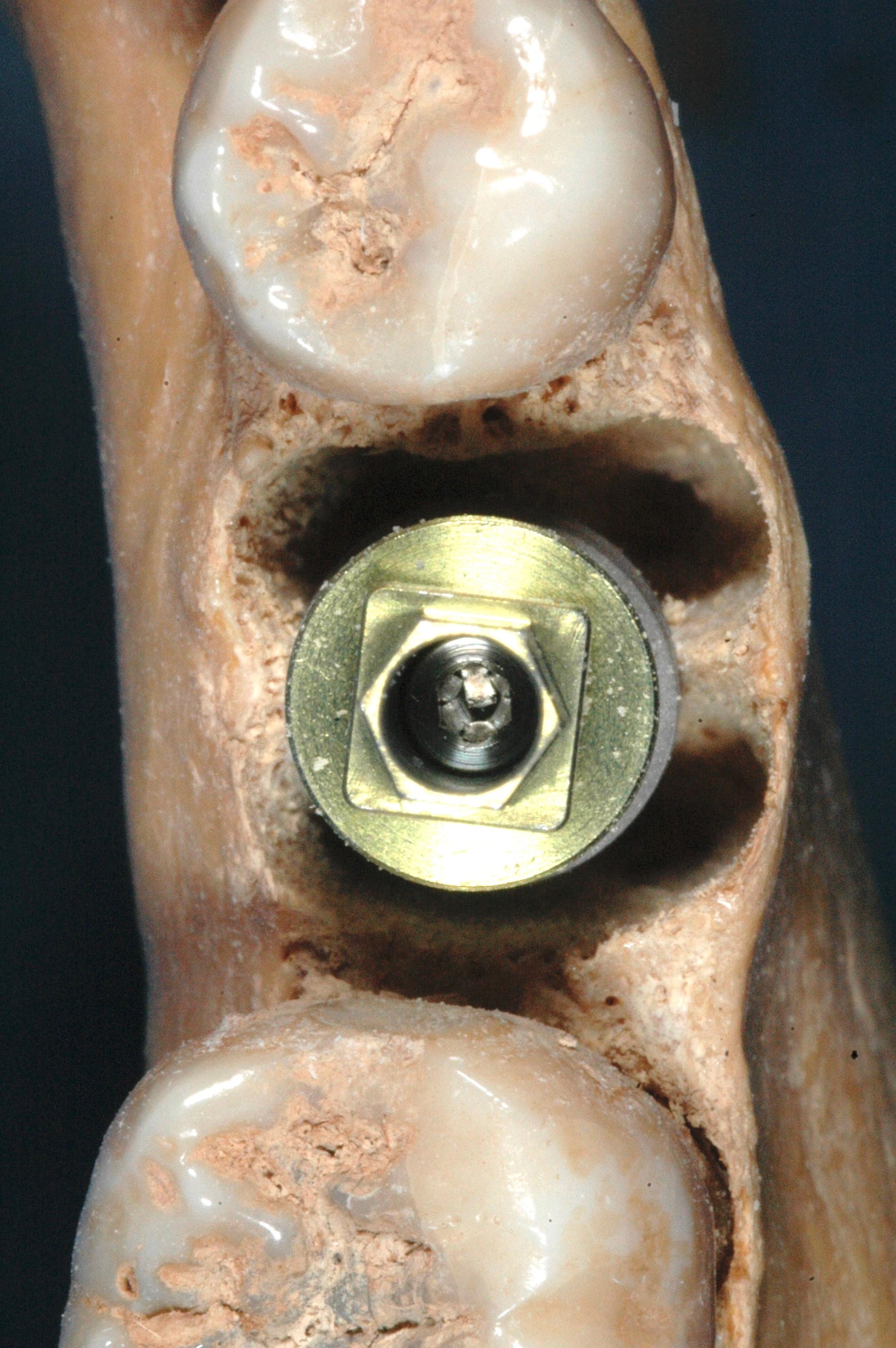
Implant placement in molar extraction sockets can be difficult due to complex multi-root anatomy and the lack of predictable primary stability. The aim of this study was to evaluate the outcome of an 8 – 9 mm diameter tapered implant, designed to be placed in molar extraction sockets.
MATERIAL AND METHODS:
Patients treated at least 1 year before with a Max(®) implant (Southern Implants, Irene, South Africa) were invited for a clinical examination. Variables collected were surgical and prosthetic protocol, implant dimension and smoking habits. Peri-implant bone level was determined on peri-apical radiographs and compared to baseline, being implant insertion.
RESULTS:
98 implants had been placed in 89 patients. One implant had failed. Thirty eight patients representing 47 implants (maxilla 26, mandible 21) were available for clinical examination. Mean bone loss was 0.38 mm (SD 0.48; range – 0.50 – 1.95) after a mean follow-up of 20 months (range 12 – 35). Implant success was 97.9%. Around 30 implants, a bone substitute was used to fill the residual space, but this did not affect the bone loss outcome. Bone loss was only significantly different between maxilla and mandible (0.48 mm vs. 0.27 mm) and between the 8 and 9 mm diameter implants (0.23 mm vs. 0.55 mm). A full papilla was present at 71% of the interproximal sites and irrespective of bone loss.
CONCLUSIONS:
The Max(®) implant demonstrated good primary stability, when placed in molar extraction sockets, with limited bone loss over time.
